Corticosteroids have been widely used as an anti-inflammatory agent to treat symptoms in a variety of diseases like COPD, asthma, allergies, fungal dermatitis and the list is never ending.
The fact that corticoids provide quick relief make us think that they’re the “wonder drug”, sort of like the jack of all trades for every condition. But we often overlook the fact that they’re basically like double edged swords. They mostly treat symptoms, not diseases, except a few rare conditions that result from corticoid deficiency.
My experience with corticoids began early in life as I have a history of allergies since childhood. Back in the day and even now I see physicians prescribing corticosteroid combination ointments for conditions like fungal dermatitis. The only thing I’ve noted is that they work well for the first few days and then once the patient stops using them, the infection returns, but now the spread seems more aggressive.
This causes frustration and the patient ends up using more of the ointment and this leads to a chronic resistant type of fungal infection, and the patient becomes dependent on steroids to control the condition. This overuse of steroids also leads to adverse effects such as stretch marks, darkening of skin etc.
Overuse of inhaled corticosteroids can lead to opportunistic infections such as candida and aspergillus and systemic corticoids have been known to cause hyperglycemia and Cushing-like symptoms, the features we commonly see in Cushing’s syndrome.
A recent example of corticosteroid abuse has been the COVID-19 pandemic. Corticoids have been used extensively even when it has only been indicated for patients requiring oxygen therapy or ventilator support. This rampant use of corticoids has lead to opportunistic infections, most commonly being mucormycosis. The image below clearly shows the pitfalls behind corticoid use.
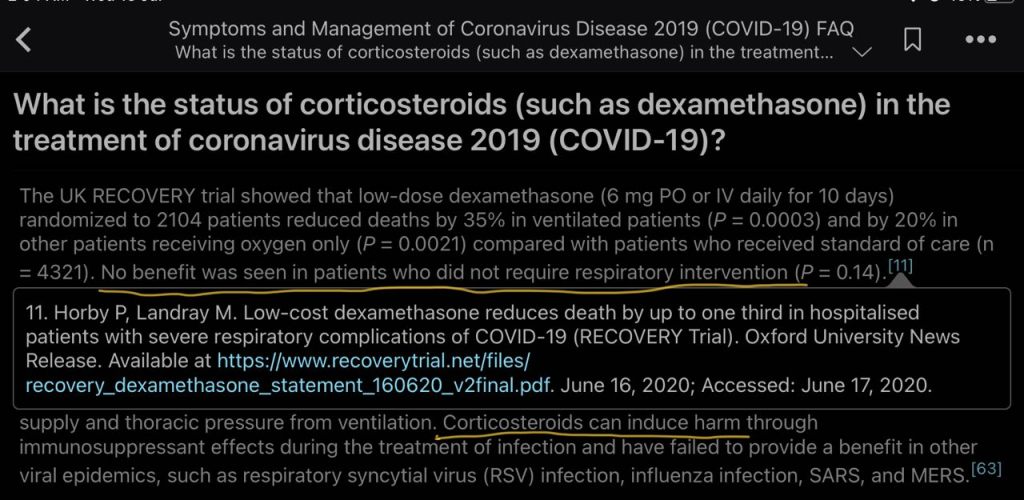
While corticoids have proven to be beneficial in conditions like COPD or Asthma requiring beta agonists such as SABA or LABA, and in patients with COVID-19 requiring ventilatory support, I believe we should clearly limit the use of this class of drugs for reserved cases only, where a clear benefit has been established.
What’s your take on this situation? Do you think corticoids have been used judiciously or do we need changes to our approach towards using them?